

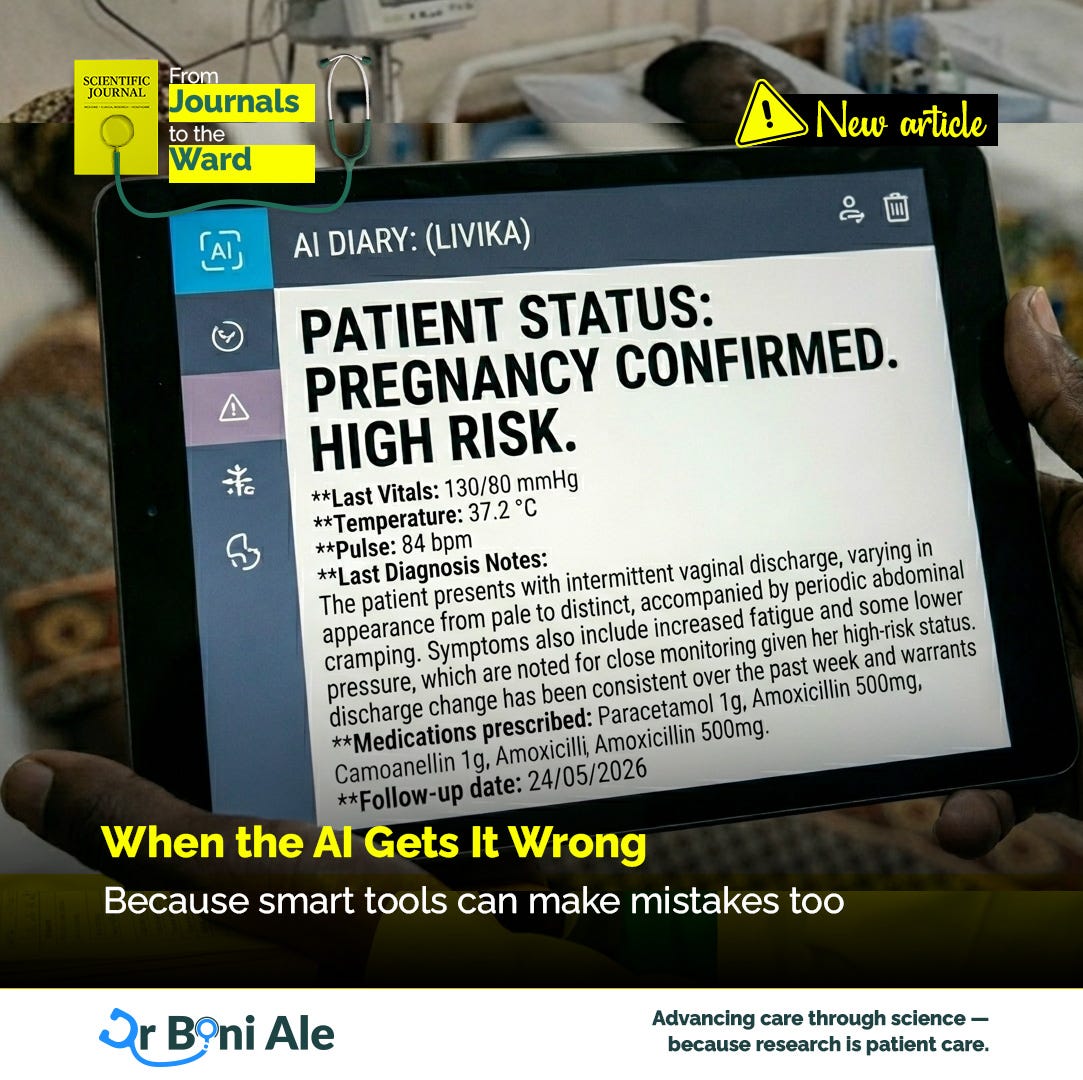
When the AI Gets It Wrong
Because smart tools can make mistakes too

AI in health care has one very impressive habit:
It is often wrong with enormous confidence.
A human colleague might say, “I’m not entirely sure.”
An AI tool says, in effect, “High risk. Recommended action. Kindly proceed.”
That confidence is part of the problem.
Because when a digital system sounds polished, fast, and certain, people can start treating it like the smartest voice in the room — even when it is making no sense at all.
And that is where clinicians need to stay awake.
Because AI can help. But AI can also get things wrong.
Sometimes subtly.
Sometimes spectacularly.
Sometimes with a neat dashboard and excellent grammar.
The danger is not just error. It is authority.
Doctors are used to uncertainty. Nurses are used to uncertainty. Patients, unfortunately, are also used to uncertainty.
But AI often presents itself without much hesitation.
It gives a score. A flag. A recommendation. A warning. It rarely says, “To be honest, I’m guessing a bit here.”
So the risk is not only that the answer is wrong.
The risk is that the answer looks official enough to stop people from questioning it.
And once nobody questions it, bad decisions can travel very quickly.
What does “wrong” actually look like?
Sometimes the AI tool says a patient is low risk when everyone in the room can see the patient is definitely not low risk.
Sometimes it recommends a next step that makes perfect sense in theory and no sense at all in your clinic.
Sometimes it misses what matters because the information it needed was never entered properly.
And sometimes it gives a recommendation that is technically tidy but clinically ridiculous.
In other words, AI can fail in the same way people fail:
by misunderstanding the situation, missing context, or sounding much more sure than it should.
The difference is that people are usually easier to interrupt.
So what should clinicians do?
The first step is simple:
Do not confuse support with authority.
An AI tool is not a senior consultant.
It is not a final verdict.
And it is definitely not a replacement for looking at the patient in front of you.
When the AI output feels wrong, pause and ask:
Does this match the patient I am actually seeing?
What information might the system be missing?
Was the input data complete and accurate?
Does this recommendation make sense in this clinic, with these resources?
If I follow this blindly, what harm could I cause?
Those questions are not anti-technology.
They are basic survival skills.
Clinicians still need to trust their discomfort
One of the most useful phrases in medicine is:
“Something about this doesn’t fit.”
That sentence has rescued many patients.
Because sometimes the numbers look calm, but the patient does not.
Sometimes the recommendation looks elegant, but the workflow is impossible.
Sometimes the screen says one thing, and your clinical judgment says another.
That discomfort matters.
AI should not replace it.
If a digital tool gives an answer that feels polished but wrong, clinicians should trust themselves enough to slow down and investigate.
Not because humans are perfect.
But because context still matters, and machines are not good at context in the way real care demands.
Policymakers and managers need to resist a different temptation
The temptation at leadership level is this:
If the system looks modern, it must be working.
That is not always true.
A smart-looking tool may still:
confuse staff
slow workflows
increase documentation burden
create new blind spots
or produce recommendations nobody trusts enough to use
So the right question is not:
“Do we have AI?”
The right questions are:
Is it helping?
Is it accurate enough?
Do staff understand it?
Do patients benefit?
What happens when it gets something wrong?
Because technology without oversight is not innovation.
It is just risk with branding.
Good AI use requires permission to disagree
This is probably the most important point.
If clinicians feel they cannot challenge the system, the system becomes dangerous.
If junior staff feel they must obey the tool even when it seems wrong, the tool becomes dangerous.
If nobody is clear about who is accountable when the AI makes a bad recommendation, the tool becomes dangerous.
Good systems do not just install technology.
They create room for people to question it.
Because safe care depends not only on smart tools, but on smart resistance.
In summary
AI can be useful. It can support decisions, highlight patterns, and reduce some repetitive work.
But it can also be wrong.
And when AI gets it wrong, the real danger is not just the mistake.
It is the confidence, authority, and speed with which the mistake enters the room.
So clinicians should do what good clinicians have always done:
Pause.
Question.
Compare.
Think.
Then decide.
Because in the end, smart tools should support judgment — not replace it.
And if a machine starts sounding more certain than the clinical reality allows, that is not intelligence.
That is just overconfidence with electricity.
Next Up: The Politics of “Best Practice”
Because not everything called “best practice” is neutral. Next week, I’ll explore who gets to define good care — and why power, money, and context often shape that answer more than we admit.